COBRA: Cone-Beam CT Reconstruction for Radiation Therapy¶
Can you turn a noisy, scatter-corrupted cone-beam scan into an image good enough to plan a radiation treatment on? That is the COBRA challenge.
COBRA is the first large-scale CBCT reconstruction benchmark to combine authentic clinical projection data with controlled synthetic evaluation. We provide raw cone-beam projections acquired during routine radiotherapy at six clinical centers, on both Elekta and Varian systems, and ask you to reconstruct volumetric images that approach the quality of the fan-beam planning CTs used to design treatments. The challenge runs on grand-challenge.org and concludes with a final event at MIDL 2027.
The Clinical Problem¶
Radiotherapy is one of the pillars of cancer treatment — used in more than half of all cancer patients at some point in their care. The workflow has a characteristic shape: a patient is imaged once on a high-quality fan-beam planning CT, a treatment plan is carefully optimized on that image, and the plan is then delivered in daily fractions over the course of several weeks.
The difficulty is that the patient on day 25 is not the patient who was scanned on day 1. Anatomy drifts over a treatment course — patients lose weight, the bladder and rectum fill and empty differently each day, bowel gas moves, tumors shrink in response to the dose already delivered. A plan that was optimal on the planning CT can become suboptimal, under-dosing the target or over-dosing a neighboring organ at risk.
The promise of adaptive radiotherapy is to correct for this: re-evaluate, and if needed re-plan, on an image of today's anatomy. And that daily image almost always exists already. Modern linear accelerators carry an on-board imager that acquires a cone-beam CT (CBCT) with the patient lying in treatment position, immediately before the beam is delivered. CBCT is ubiquitous precisely because it is convenient — no extra appointment, no moving the patient, no separate scanner.
The catch is image quality. CBCT is excellent for what it was designed to do — verifying patient position by aligning bony anatomy — but its image quality has historically been too poor to plan a treatment on and more importantly for image assessment or target/organ segmentation. Closing that quality gap is the problem COBRA puts in front of you.
CBCT Reconstruction Is Hard¶
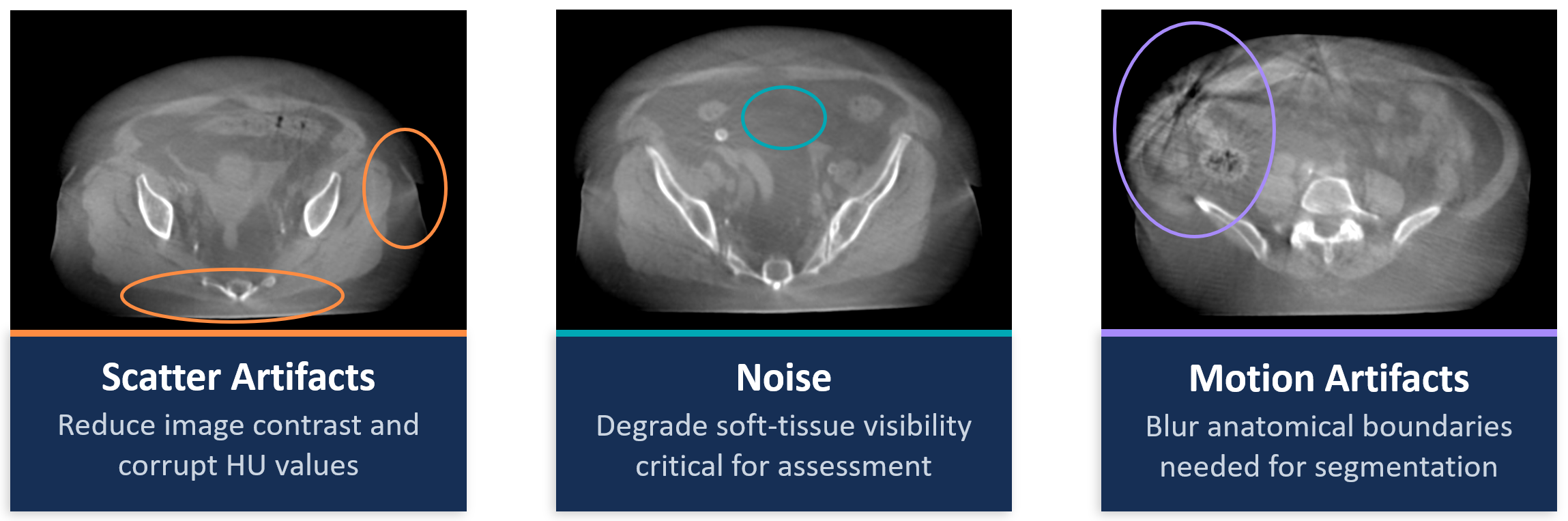
A cone-beam acquisition is a fundamentally harder inverse problem than diagnostic fan-beam CT, and the resulting artifacts are not cosmetic. They corrupt the Hounsfield units (HU) that radiotherapy dose calculation depends on, and they degrade exactly the soft-tissue detail that matters for targeting. Four obstacles dominate:
-
Scatter. The large cone-beam geometry illuminates a big volume at once and a flat-panel detector collects an enormous quantity of scattered photons alongside the primary beam. Unlike the well-collimated fan-beam case, this scatter is large, spatially varying, and object-dependent. It manifests as cupping and shading across the image and can shift HU values by hundreds of units — enough to make a dose calculation clinically meaningless if uncorrected. Scatter correction is the single biggest lever in CBCT quality.
-
Noise. CBCT typically delivers less dose per projection than a planning CT, so quantum (photon-counting) noise and electronic detector noise are far more prominent. The result is poor soft-tissue contrast — and soft tissue is precisely where tumors and organs at risk live. Suppressing noise without erasing genuine low-contrast structure is a delicate balance.
-
Motion. A CBCT acquisition takes anywhere from a few seconds to about a minute as the gantry rotates. In the thorax and upper abdomen, respiratory motion during that window blurs edges and introduces motion streaks. Even in the pelvis, peristalsis and involuntary motion perturb the reconstruction.
-
No clean ground truth. This is the subtler obstacle, and it makes evaluation hard rather than just the task. The planning CT and the CBCT are acquired days — sometimes weeks — apart, so the underlying anatomy has genuinely changed between them. There is no pixel-perfect reference image for a real clinical scan, even in principle. Deformable image registration narrows the gap by warping the planning CT onto the CBCT anatomy, but residual mismatch always remains, especially in deformable soft tissue and gas-filled regions. Any honest evaluation has to be designed around this limitation rather than pretend it away — which is exactly why COBRA pairs real data with simulated data that does have known ground truth.
Potential¶
If a reconstruction can reach planning-CT quality — accurate HU for dose, faithful geometry for targeting — then the daily in-room CBCT becomes a re-planning image which can be also used for assessment. Adaptation happens on the scan you already have: no additional CT, no additional dose, no additional appointment, and a plan that tracks the patient's anatomy fraction by fraction. For a workflow that touches half of all cancer patients, even incremental gains compound into large clinical benefit.
Scatter correction, noise reduction, and motion management are long-standing problems across the whole of cone-beam imaging. COBRA frames them on standard linacs already installed in clinics worldwide, so methods that win here are methods that can deploy without new hardware. Advancing the state of the art on authentic, multi-vendor clinical data — rather than on a single simulated benchmark — is the technical contribution the challenge is built to produce.
The Task¶
You are given a stack of CBCT X-ray projections together with the acquisition geometry (gantry angle per projection, source–detector and source–origin distances, detector offsets, and imaging parameters), and you reconstruct a volumetric image that is as close as possible to planning-CT quality — accurate in both intensity (Hounsfield units) and geometry (anatomical fidelity).
Methods must be fully automatic. The algorithm should behave like a traditional reconstruction pipeline: projections and geometry in, a reconstructed volume out, with no manual intervention, no case-by-case tuning, and no interactive steps. This mirrors how a reconstruction algorithm would actually be deployed in a clinic.
The challenge provides two complementary data types, and the strongest submissions will need to perform well on both:
| Real-world data | Synthetic data | |
|---|---|---|
| Input | Clinical CBCT projections from routine treatments | Physics-simulated projections from planning CTs |
| Reference | Deformably-registered planning CT | Known ground truth (the deformably-registered CT) |
| Strength | Authentic artifacts, real clinical variability | Perfect alignment, fully controlled evaluation |
| Limitation | No perfect ground truth | Simulation cannot fully capture real artifacts |
Each data type answers a question the other cannot. Real data is the only honest test of whether a method handles the messy, vendor-specific, patient-specific artifacts of clinical practice — but it can never be evaluated against a perfect reference. Synthetic data gives organizers a controlled setting with known ground truth and clean, repeatable evaluation — but a simulation is only ever an approximation of reality. Together they let participants develop on realistic data while organizers evaluate under rigorous, controlled conditions. This pairing is what bridges the usual gap between academic benchmark performance and clinical deployment.
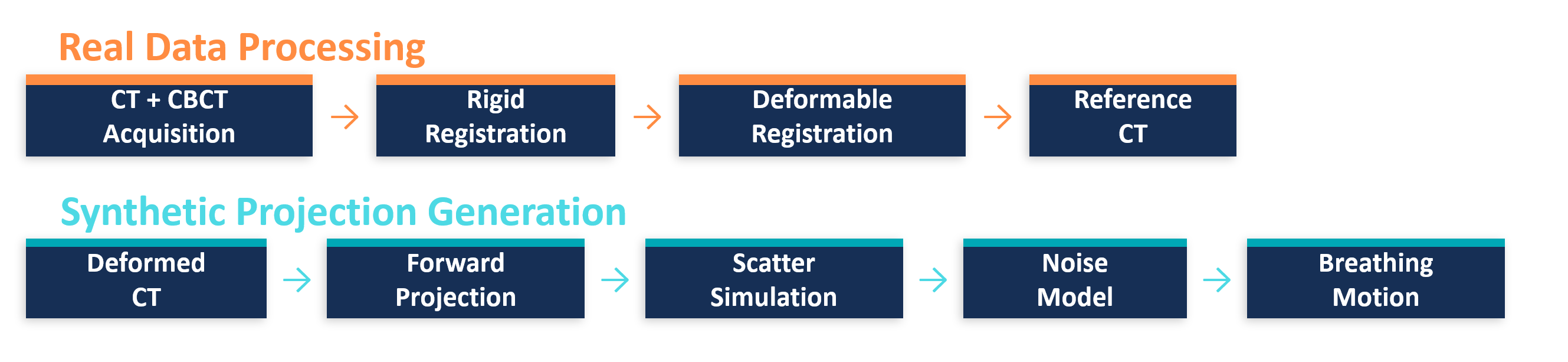
The simulated projections are generated from each registered planning CT through a realistic pipeline: analytical forward projection on the true scan geometry using custom CUDA ray-tracing; a heuristic scatter model driven by primary counts and scan parameters (mA, ms) with a scatter-to-primary ratio defined per scanner geometry; compound Poisson–Gaussian noise combining dose-dependent quantum noise and electronic noise, calibrated to clinical noise levels; and periodic breathing motion modeled with deformation fields at typical respiratory periods of 3–6 seconds and superior–inferior amplitudes of 2.5–7.5 mm. Because a simulated case is produced for every patient, the dataset effectively doubles.
Get Involved¶
Registration opens alongside the training data on 13/07/2026. From there, the Data, Submissions, and Metrics & Ranking pages have everything you need to build and test a method, and Timeline & Rules lays out the schedule, eligibility, and award policies. Questions are welcome in the Forum.
We hope you enjoy taking part in COBRA.
— The COBRA organizers